A. Donà | G. Porcellini | M. Novi | M. Delvecchio | G. M. Micheloni | A. Giorgini | L. Tarallo | I. Baldelli
Introduction
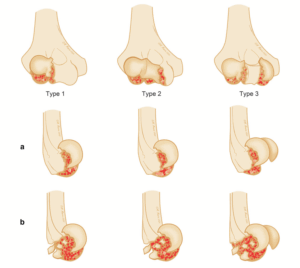
Poland syndrome (PS) is a rare congenital malformation characterized by agenesis or hypoplasia of pectoralis major muscle. The most common feature is the absence of the sternocostal head of the pectoralis major muscle with concomitant hypertrophy of the clavicular head and the absence of the pectoralis minor; other manifestations often associated are ipsilateral hand and upper limb anomalies, such as syndactyly, absence/hypoplasia of the breast and rib aplasia (Fig. 1) [1–4].
Although the syndrome usually occurs unilaterally, some cases of bilateralism have been observed [5–7].
The incidence of Poland syndrome has been reported to be approximately one in 30,000 live births [8], with a higher prevalence in males (M/F 3:1) and with the right side of the pectoralis being affected more frequently [3, 7].
The etiology underlying Poland syndrome is still unknown. A vascular disruption due to a hypoplasia of subclavian artery during the 6th week of gestation remains the most accepted pathogenic mechanism. The theory suggests that the interruption of the embryonic blood supply causes hypoplasia of the ipsilateral subclavian artery or one of its branches. This results in muscle absence and variable clinical manifestations in areas supplied by the artery [9].
Other risk factors that seem to be involved are smoking or cocaine abuse in pregnancy [10–12]. The diagnosis of Poland syndrome is still mostly clinical. The unilateral agenesis or hypoplasia of the pectoralis major muscle is assessed by a clinical test, asking to the patient to push the palms of the hands against each other with the arms flexed anteriorly. Most patients live a normal life, carrying out daily activities and even practicing sports and exercises. In most cases, reconstructive surgery is required by patients only for cosmetic reasons: In fact, during the pubertal development, the asymmetry of the thoracic region in males or of the mammary region in females become more evident and can cause discomfort, leading to a reduction in the quality of life [13–15].
Functional limitations of these patients are usually minimal, as demonstrated by the presence of Poland syndrome in athletes [16]. Actually, there is a limited literature on how the anatomic anomalies of PS may impact the movement of the shoulder both functionally and biomechanically. The study of shoulder range of motion (RoM) using wireless inertial motion capture devices showed a high accuracy and reliability [17–19].
Currently, though, there are no studies on the impact of the Poland syndrome on the biomechanics and the ROM of the shoulder. Aim of this study was to analyze the effects of the absence of the pectoralis major and minor muscles on the kinematic of glenohumeral and scapulothoracic joints in the life span, among a cohort of patients affected by Poland syndrome. The hypothesis was that even if the RoM of the shoulder do not differ, scapular motion on the pathological side significantly differ from healthy side. The research evaluated clinical aspect such as range of motion (RoM), joint instability, muscle compensation, rotator cuff alteration and the possible alteration of the scapular kinematics by motion sensors acquisitions.
Clicca sul pulsante sottostante per continuare nella lettura dell’articolo completo e visualizzare le immagini di approfondimento.